
It had been a rough week and I was questioning what I was doing with SNR and how I was going to pull off a very lofty set of personal, professional and community goals amidst all the other things going on in my world and the world around me.
All it took for me to turn the ship around was a phone call from someone who needed my help. I don’t have a God complex (I can’t save you) and I don’t have an overinflated ego (it is appropriately inflated). I do find purpose and meaning in helping others, but I had the honor of providing the person on the other end of the call something that they had been struggling with …
Hope.
When the prognosis is poor or uncertain, we crave it. When we are fighting battles – whether they are medical, societal, emotional, or other, we build with hope. We seek it when we need to keep going.
Through my own life experiences, I have ridden the rollercoaster of hope. That one time I thought I was going to die and the doctor said, “If you’re going to have cancer, this is the kind to get…”(Weird way of putting it, but ok.) The time that the young, naive romantic in me saw a lingering glance of a first love and thought, “Maybe we can make it work.” (We couldn’t). The time I held my newborn… (twice). The time when my dad moved his hand in mine when he was in the ICU and I was convinced the neurologist had to be wrong about him being braindead because he moved his hand… (He was 100% right- dad was gone).
Hope isn’t always a gain/lose scenario. In my experience (as noted above), it is more of a rollercoaster with highs and lows. In dealing with medical disorders, diseases and deficits, I have seen how hopeless a patient/parent of a patient can get. Practitioners and clinicians are not hope dealers. It isn’t our fault; we have to be straight forward and give our best clinical impressions along with worst case scenarios. We can’t candy coat it or provide all the possible rights because the odds aren’t ever in our favor.

As practitioners and clinicians, however, we don’t always have to crush diagnostic hope. To me, diagnostic hope is where the doctor tells you your odds, identifies limitations, provides labels and gives you options.
Over the years, I have heard so many patients be relegated to their disease or disorder through the destruction of diagnostic hope. In reviewing statistics, discussing with experienced clinicians, completing evaluations, going through research etc, we can identify that the odds are stacked against a patient. But who are we to say they won’t be the one exception to the rule? Who are we to say we are not going to get anywhere based on first glance, second glance, or even 14th glance?
The great unknown variable in any rehabilitative scenario is the individual. In order to treat the individual, you have to be able to provide them with some form of hope. You have to give them a goal, you have to provide them with support. You have to let them know they aren’t crazy, they aren’t alone, and there are ways to keep going.

Maybe we should look at including a component of our professional practice as hope dealers – finding the silver lining and highlighting it with one of those gel highlighters that will NEVER come out if you get it on your clothes. I am not saying that you should say, “Everything happens for a reason, ” (Don’t. Ever. Really. Just don’t say it. That is not the thing to say to a person in crisis or coming out of crisis. I promise you, as a thoroughly traumatized person myself, I can attest that it can earn you a swift throat punch if said to the wrong person at the wrong time).
Just in that one phone call, I empathized. I said, “I understand.” I identified that their concerns and frustrations were valid, and I offered to help in any way I could. That made all the difference for them. In the time that they have struggled, they haven’t felt heard or fully understood. They can now look at the situation with a little hope, where before there was desperation and helplessness.
In turn, it gave me hope that in continuing to travel this road, I am on my way to reach the goals I have set for me. My gift is the type of therapeutic intervention I can provide. I will use my gift to spread hope along with the tasks, strategies, supports and education I can provide my patients.
In my daily life, I will try to consider the diagnostic hope that hides in every poor standardized score, every indicator of deficit, difficulty or decline. I will try to use it to be a hope dealer. I have had many a hope dealer in my life, and I want to be sure to pay it forward to the people I serve.
 On a much less important scale, I have hope for Rainier cherries to be at Costco soon. They are my favorite fruit.
On a much less important scale, I have hope for Rainier cherries to be at Costco soon. They are my favorite fruit.
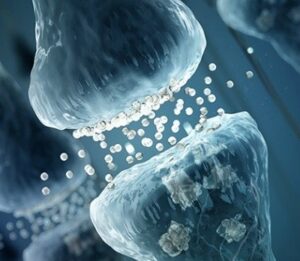 A synapse is the moment in the brain where two neurons connect and pass messages to each other. We create these as we learn and grow throughout our lifetimes. These synapses create the thoughts, the movements, and actions that we need to complete basic life functions.
A synapse is the moment in the brain where two neurons connect and pass messages to each other. We create these as we learn and grow throughout our lifetimes. These synapses create the thoughts, the movements, and actions that we need to complete basic life functions.